The Coronavirus Endgame: How the pandemic ends, and how we get there

MichaelMaggs / CC BY-SA (https://creativecommons.org/licenses/by-sa/2.5)
{Thirteen months later in May 2021, I published a final Endgame essay.}
This is my longest, most challenging, and most important coronavirus series. Part 1 of 4. Please read, and please share.
The Coronavirus Endgame:
The end of the COVID-19 / SARS-CoV-2 coronavirus pandemic, and how we’ll get there
We’ve spent the last several weeks wrapping our heads around the idea of a pandemic. For those of you who did not share my long-term, macabre fascination with microorganisms and historic plagues, the emergence of a new virus and its shockingly fast spread to every region of the globe probably was hard to believe. Who could have imagined it? Well, lots of people did, including both scientists and science fiction writers.
The shock is dissipating. I think we have gotten somewhat used to the fact that COVID-19 exists, and to the idea of stay-at-home orders. Humans are adaptable creatures. Our thoughts are now shifting ahead, toward the coronavirus endgame. SARS-CoV-2 entered our lives in a dazzling flash. How will it leave?
It might not.
You know, I’m reminded once again how much life is imitating art these days. The real world is grappling with a plot problem I talk about when I give lectures on the craft of science thriller writing. I call it the “killer virus” problem.
For novelists, the “killer virus” problem is the question of how to wrap up a story in which a deadly infectious agent has been released into the story-world. It’s not easy. The author basically must choose between scientific verisimilitude and an emotionally pleasing resolution. In other words, happy endings aren’t plausible. You can’t set a plague loose on your story-world and then erase it in a few pages; that’s not how pandemics work. Many thriller writers choose the happy ending regardless, tossing a miraculous cure or an instantly available vaccine into the plot. {The alternative is to write a story where suspense is focused on preventing the release of the virus; or to write a dystopian tale about what happens after the pandemic. In my own books, I go to great lengths to establish a scientific backdrop that allows for partial or limited release of the agent, so that a happy ending doesn’t betray my tech principles.}
So what ending will our “killer virus” story have?
As the pain of social distancing mounts, it is dawning on people that they don’t understand where we’re going with this. They may have been under the impression that the shutdown is a way to “beat” the virus. It is not. The shutdown is not a weapon to defeat coronavirus. It is a siege battle, where we lock ourselves behind a wall and our enemy circles around us. From our place of safety, we use the time to build a catapult.
**********
There’s a saying in medicine: all bleeding stops eventually. Same with pandemics. The dynamic relationship between hosts and virus eventually settles into a new normal. Right now, our relationship with SARS-CoV-2, the new coronavirus that causes COVID-19, is totally unstable. Today, we are immunologically naive, easy prey for the virus. But over time the power balance between it and us will shift. How will it end? And are we mere spectators, or can we choose our path to get there?
Victor or vanquished?
For any emerging virus, in the long term there are three possible outcomes:
- Humans go extinct; virus wins.
- Virus disappears; humans win.
- Equilibrium; both humans and virus persist with a somewhat constant level of warfare.
Which will happen with the coronavirus SARS-CoV-2?
#1 is not a possibility — not with this virus. Remember a long time ago (like, February) when we were debating whether the new coronavirus was even a problem we should bother about? That’s partly because we didn’t know the mortality rate — the percent of infected people who die of the infection. We still are painfully short on data to pin this down, but based on public data the highest conceivable number is 5% (and I guarantee it’s lower than that). 5% is a devastating number of people, but it’s not an extinction-level event. SARS-CoV-2 is not a slatewiper. It’s no smallpox or even Ebola. This virus does not pose an existential threat to our species.
#2 is a fantasy Trump endorsed on Feb. 27 when he said, “One day it’s like a miracle, it will disappear.” The president was widely criticized for this ill-timed and counterproductive claim, but guess what? Some viruses truly do just disappear, as if by magic. The 1918 pandemic flu did, eventually. So did the original SARS virus, helped along by human efforts at containment. And zika — where did it go? We can hope for such a miracle with the new coronavirus, but the odds are not good. Maybe summer will bring a reprieve. Flu pretty much goes away in the summer, but that’s partly due to our existing immunity to flu. Against coronavirus, we have none. It’s virtually impossible that our own containment efforts, no matter how drastic, can put this virus genie back in the bottle. The most likely endgame is…
#3: Equilibrium. SARS-CoV-2 becomes a fixture in our microbiologic environment, waxing and waning, maybe seasonal, always a threat. An ongoing guerrilla war between us and them is the pattern for all the disease-causing viruses that have been with us for a while — influenza, measles, chickenpox, HIV, polio, hepatitis A, the common cold. We’ve gotten used to the equilibrium being mostly in our favor because of vaccines. Drug treatments, behavior modification and sanitation have also allowed most of us to ignore these viruses and live our “normal” lives. Each of these viruses claims a certain number of human lives every year, generally in a predictable range of fatalities. One way or another, the coronavirus curves will flatten, and we’ll arrive at an armistice. Deaths will stabilize; at what level remains to be seen.
I’m defining “equilibrium” as a time when our collective behavior is sustainable for the long term (i.e., not on lockdown) yet we don’t have any explosive spike in deaths. Like with influenza, in coronavirus equilibrium a consistent number of people will regularly perish due to infection. Any surge is seasonal or circumstantial.
Stalemate: Reaching equilibrium
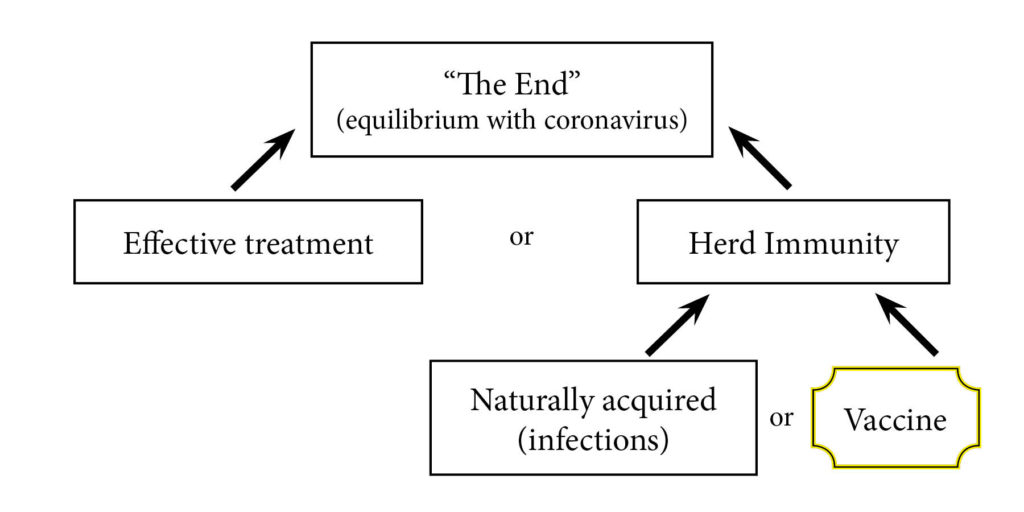 There are only two ways to reach equilibrium:
There are only two ways to reach equilibrium:
- an effective, widely available treatment for COVID-19 disease; or/and
- population-level immunity (herd immunity) against the coronavirus
If we stumble on a recipe for a treatment regimen that dramatically improves the survival of patients stricken with COVID-19, we could resume normal life without fear of a spike in deaths. A spike in cases, yes, but not deaths. Such a treatment would have to be scalable, meaning our health care system could deliver the treatment to a very large number of people at once. If a drug is involved, that means manufacturing it in large quantities.
Realistically, it’ll be very hard to meet these criteria. Even if an effective therapy is quickly found (a big “if”, see my post on why we have so few antiviral drugs), we will probably have to continue social distancing to slow the rate of infection. A spike in cases could overwhelm the health care system or use up the supply of a new drug, denying COVID-19 patients the care they need.
Herd immunity is the most likely path
The other path to equilibrium is population-level immunity, often called herd immunity. To understand herd immunity, imagine a wildfire in a forest. The fire is a virus. It infects one tree, increases itself, then spreads to the next tree. If the trees are dry and crowded, the fire spreads fast and gets very hot. But if some of the trees are wet and fire-resistant, the fire can’t infect them. If enough of the trees are immune to fire, the fire spreads slowly or even dies out.
People who have immunity against a virus are like wet trees in a forest of flammable folks. When their numbers are great enough, the fire diminishes or extinguishes, saving the dry trees from destruction.
According to public health experts at Johns Hopkins University, based on the infectiousness of SARS-CoV-2, “we will likely need at least 70% of the population to be immune to have herd protection.” The US population is about 325,000,000, so 70% is about 225,000,000 people.
How do 225 million people acquire immunity to SARS-CoV-2? There are only two ways:
- immunity acquired naturally through infection, or
- immunity through vaccination.
And so you see the great dilemma before us. Our final destination is herd immunity. To get there, should we choose the path of vaccination? Sure, except we don’t have a vaccine. I am hopeful we will, but it’s possible a vaccine will elude us (see: HIV). Under even the best circumstances, identifying, testing, manufacturing, and distributing a vaccine to 225 million Americans (not to mention billions around the world) will take time — probably over a year. Too long for society to survive the economic paralysis of lockdown.
Okay, so then should we choose immunity via natural infection? In other words, end social distancing and let ‘er rip? Sure, except a lot of people will die, including many who don’t even have COVID-19 but are squeezed out of the health care system by a surge of COVID patients.
The cost of lockdown is staggering, so it’s fair to ask, how many lives are we protecting as we hold out for a vaccine? The trillion-dollar question is, if we allow the virus to spread and reach herd immunity naturally, how many would die of COVID-19?
The mortality rate for SARS-CoV-2 is still not known with precision. Using only cases that are formally diagnosed, the case fatality rate worldwide is in the range of 5%. However we know that a large number of cases are not tested or diagnosed, and this increases “the denominator.” A few days ago, Stanford released data from a serology study of a sample of people in Santa Clara County, CA. They estimate the actual number of people who have been infected with the virus is 50–85 times higher than the diagnosed case count. As a consequence, they estimate the mortality rate at 0.1 to 0.2% for people in Santa Clara County.
So how many Americans would die on the way to natural herd immunity? With that range of uncertainty, one can plausibly argue for a number anywhere between 200,000 and >10 million. For reference, in 2017 in the US, 600,000 people died of cancer and about 650,000 of heart disease.
Natural infection for some, wait for a vaccine for others?
Fortunately our path doesn’t have to be either/or. No credible leader in America today has put forth a plan to reopen the economy without any restrictions. Both federal and state-group plans combine some reopening with some distancing and public health efforts to slow the epidemic and buy more time for the vaccine option. In this way, we could slowly increase herd immunity via natural infection while also protecting the most vulnerable in hopes that they can eventually be vaccinated.
As with every choice in this difficult situation, loosening restrictions is risky. The virus could surge out of control. Some people will die. On the other hand, staying locked down isn’t only costly, it’s a gamble on a vaccine or cure, neither of which is guaranteed. If a vaccine or cure never comes, herd immunity is the only endgame, and social distancing becomes (mostly) a waste of effort and money. Flattening the curve — spreading out COVID-19 deaths over time — saves non-COVID patients who need to use hospitals, but it doesn’t significantly decrease the cumulative number of people who will die of COVID itself. Lives can be saved from coronavirus only by a treatment or a vaccine. Social distancing only buys time.
The great debate about how to soften social distancing has begun. At its core, this is an argument about the path we wish to take to herd immunity. Herd immunity acquired the hard way, through natural infection, is the only guaranteed path to equilibrium (and the end of the pandemic). The alternatives are a treatment or a vaccine — shortcuts that are greatly desirable, but uncertain of timing or success.
Coronavirus Endgame PART 2: The truth about nonpharmaceutical interventions, or, why social distancing won’t save us
Amy Rogers, MD, PhD, is a Harvard-educated scientist, novelist, journalist, and educator. Learn more about Amy’s science thriller novels, or download a free ebook on the scientific backstory of SARS-CoV-2 and emerging infections, at AmyRogers.com.
Sign up for my email list
0 Comments
Share this:
0 Comments